Diabetes: The Biggest Threat to Mankind – An Indian Perspective
India is facing an unprecedented health emergency. Recent data confirms that over 101 million Indians are living with diabetes, with another 136 million—more than the population of most countries—already in the pre-diabetic stage. This blog post examines the scale of the crisis, the unique challenges Indian patients face, the economic burden on families, and practical, culturally-appropriate strategies for prevention and management.
ASF
2/23/20268 मिनट पढ़ें
India finds itself at a critical juncture. On one hand, we are a nation celebrated for our economic growth, technological prowess, and a demographic dividend that promises a bright future. On the other hand, we are silently battling a monster within—a metabolic mayhem that threatens to cripple our healthcare system, drain family finances, and cut short the lives of millions. This monster is diabetes.
We are no longer just the "Diabetes Capital of the World"; we have become the epicentre of a global health crisis. Recent data paint a picture so alarming that it demands immediate attention from every Indian citizen, from policymakers in Delhi to homemakers in small towns. This is not merely a health issue; it is a national security and economic emergency in the making.
The Alarming Numbers: A Reality Check
Let us begin by confronting the hard facts. For years, we have heard about the rising tide of diabetes, but the latest numbers suggest the dam has already broken.
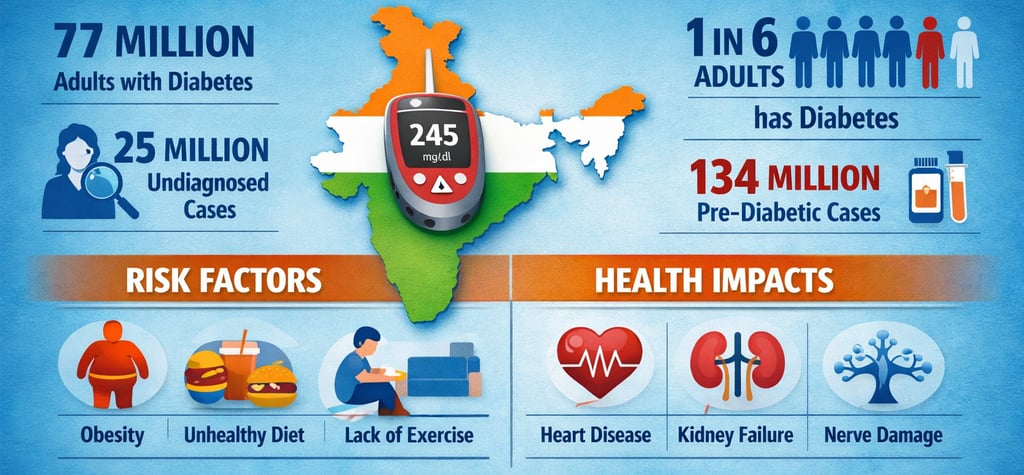
According to the recent ICMR-INDIAB study, one in four Indians is now either at risk of developing diabetes or is already living with it. The study estimates that approximately 101 million people in India have diabetes. To put that into perspective, that is more than the entire population of Germany.
Even more terrifying is the pool of 136 million people who have prediabetes. These are individuals whose blood sugar levels are higher than normal but have not yet crossed the threshold into diabetes. They are standing on the edge of a cliff, and without immediate lifestyle intervention, up to 30% of them will develop diabetes within three to five years. The Minister of State for Science & Technology, Dr. Jitendra Singh, recently highlighted this in the context of the 2026 Budget, noting that the country has over 11–12 crore diabetics and nearly 14 crore pre-diabetics.
What is most concerning is the shifting demographics. Diabetes is no longer a "rich man's disease" confined to urban elders. It is rapidly consuming the rural population and, more tragically, the young and productive middle class.
The Indian Paradox: Why Are We So Vulnerable?
To understand why diabetes poses such a significant threat in India, we must look beyond the generic causes of poor diet and sedentary lifestyle. A unique "Indian Paradox" is at play.
1. Genetic Disposition: The "Thin-Fat" Indian
Indians have a genetic predisposition to insulin resistance. We tend to have higher body fat percentages and more visceral fat—the dangerous fat that surrounds our internal organs—even at a lower body mass index (BMI) compared to Caucasians. This phenotype, often called the "thin-fat" Indian, means we can be metabolically obese even when we appear lean, making us susceptible to diabetes at a younger age and lower body weight.
2. Dietary Shifts: The Carbohydrate Overload
The traditional Indian diet, while diverse and flavourful, is often heavily skewed toward carbohydrates. Rice in the South and East, wheat in the North—our plates are dominated by carbs. While our ancestors burned this energy through physical labour, the modern sedentary Indian office worker does not.
As food environment studies have noted, urbanisation has led to a surge in the availability of processed foods and fast-food outlets, while access to fresh, whole foods has become increasingly challenging in metropolitan areas. We have adopted the worst of the Western diet—sugary drinks and processed snacks—while retaining our carb-heavy staples, creating a perfect storm for metabolic dysfunction.
3. The Reversal of Traditional Eating Patterns
Ironically, our ancestors often ate in ways that mimicked modern intermittent fasting due to seasonal scarcity. Today, we have transitioned from feast-fast cycles to continuous feasting. The concept of "eating to live" has been replaced by "living to eat," with constant snacking and high-calorie intake driving our pancreases to exhaustion.
The Economic Shock: A Burden on Families and the Nation
Diabetes does not just hurt; it costs. The economic burden of diabetes in India is the second highest in the world, trailing only behind the United States. A study published in Nature Medicine estimated the economic burden of diabetes in India at a staggering USD 11.4 trillion (international dollars) when accounting for the loss of informal care.
Why is the economic impact so massive? It stems from three factors: the sheer size of our affected population, the high cost of treatment relative to income, and the loss of productivity.
An umbrella review published in the International Journal of Diabetes and Technology attempted to estimate the annual per-patient cost of diabetes care in India. The preliminary estimate arrived at approximately ₹20,660 per patient per annum. However, this figure likely underestimates the true out-of-pocket expenses.
For a family, this translates to:
Direct Medical Costs: Doctor consultations, medications (both oral drugs and insulin), monitoring equipment (glucometers, test strips), and regular laboratory tests (HbA1c, lipid profiles).
Direct Non-Medical Costs: Transportation to clinics, special dietary foods, and hospital stays for complications.
Indirect Costs: Lost wages due to illness and time taken off by family members to care for the patient, as well as premature death.
For a daily wage worker or even a lower-middle-class family, a diabetes diagnosis can push them into a debt trap. The high share of informal caregiving—comprising almost 90% of the total economic burden in some estimates—explains why families are stretched thin, with caregivers often dropping out of the labour market.
Recognizing this financial toxicity, the Union Budget 2026–27 attempted to address the issue through the ₹10,000 crore Biopharma Shakti initiative. By boosting domestic manufacturing of biologics and biosimilars, the government aims to make drugs more affordable and reduce the long-term financial burden on families dealing with chronic diseases like diabetes.
The Clinical Reality: From Prediabetes to Complications
The journey from being healthy to diabetic is often silent, which is precisely why it is so dangerous.
Understanding Prediabetes
Prediabetes is your body's final warning shot. It is generally asymptomatic, though some people may experience slight tiredness, blurred vision, or increased urination. The key numbers to monitor are HbA1c, fasting blood sugar, and post-meal blood sugar. An HbA1c ranging between 5.7% and 6.4% indicates prediabetes. This represents the "golden window" of opportunity. Long-term studies have demonstrated that losing 5-7% of body weight and decreasing caloric intake can reverse prediabetes and prevent its progression to diabetes.
When Diabetes Takes Hold
Once diabetes sets in (HbA1c ≥ 6.5%), the focus shifts to management and prevention of complications:
Microvascular Complications: Damage to small blood vessels, leading to retinopathy (blindness), nephropathy (kidney failure requiring dialysis), and neuropathy (nerve damage resulting in loss of sensation and foot ulcers).
Macrovascular Complications: Damage to large blood vessels, leading to heart attacks and strokes. This is why diabetes is a major risk factor for cardiovascular disease.
The goal of management is to maintain HbA1c around 7% for most adults, with fasting glucose between 80–130 mg/dL and post-meal glucose below 180 mg/dL.
Beyond the Clinic: The Case for Community Action
One of the biggest mistakes in the fight against diabetes is assuming it can be won in the doctor's clinic alone. A 15-minute consultation can diagnose high blood sugar and advise lifestyle changes, but true behaviour change rarely begins and ends within that brief window.
Food practices in India are deeply rooted in religion, culture, and tradition. When a doctor tells a patient from a rural background to "eat better," what does that actually mean for someone whose food world begins and ends with rice and dal? This is where the healthcare system needs to evolve.
We need a partnership model:
Doctors detect risk early, explain the science of metabolism, and set clear targets.
Frontline workers (such as ASHA workers and community health volunteers) translate this guidance into practice by reinforcing nutrition education in local languages, suggesting affordable and locally available protein options (eggs, pulses, dairy, fish), and following up repeatedly with empathy.
The Urban Environment: Are Our Cities Making Us Sick?
Our living environment plays a substantial role in the diabesity epidemic. A study conducted in Chennai, published in the Journal of Diabetology, examined the association between food and physical activity environments and diabesity (the co-occurrence of diabetes and obesity).
The study found a diabesity prevalence of 32.5% among adults in the surveyed wards. Key risk factors included:
High Retail Food Environment Index (RFEI): This indicates a higher density of fast-food outlets and processed food sellers relative to healthy options like vegetable vendors.
Distance to Spaces for Physical Activity: The farther people lived from parks, green spaces, or walkable areas, the higher their risk.
Physical Inactivity: Those who were inactive had a significantly higher risk.
This serves as a clarion call for urban planners. We need cities that promote health—with more pedestrian-friendly streets, parks, and markets selling fresh produce, rather than just more fast-food joints.
Managing Diabetes the Indian Way: A Practical Guide
Managing diabetes in India requires a strategy that works with our culture, not against it. You don't have to eat tasteless food to control your blood sugar.
Building the Indian Diabetes Plate
A simple visual rule can help you design every meal:
Fill Half Your Plate with non-starchy vegetables: Think bhindi, lauki, cabbage, leafy greens, and salads.
Fill One-Quarter with protein: This could be dal, chana, rajma, paneer, soya chunks, fish, or chicken.
Fill One-Quarter with quality carbs: Opt for whole wheat roti, brown rice, parboiled rice, or millets (jowar, bajra, ragi, foxtail millet).
Regional Variations
North Indian: Swap one roti for a mix of whole wheat and besan (chickpea flour). Add a generous helping of sabzi and a bowl of dal or raita.
South Indian: Idlis and dosas can be made healthier by adding more urad dal. Replace a portion of white rice with millets or parboiled rice, and always pair it with sambar (which is packed with lentils and vegetables).
East Indian: Enjoy fish curry, but balance the rice intake with plenty of green leafy vegetables (saag).
West Indian: Jowar and bajra rotis are excellent low-GI options. Pair them with vegetable subzi and a bowl of moong dal.
The Truth About Sugar
Considerable confusion surrounds jaggery, honey, and brown sugar. Despite their "healthy" image, they raise blood glucose similarly to table sugar. They are still "free sugars" and should be limited. A simple victory? Cutting just one teaspoon of sugar from your tea or coffee twice a day saves roughly 8–10 grams of sugar daily—that amounts to 240–300 grams less sugar per month.
Smart Cooking Strategies
Cook Rice Al Dente: Overcooked rice has a higher glycaemic index.
Cool and Reheat: Cooling cooked rice or potatoes increases resistant starch, which is harder to digest and has a lower impact on blood sugar.
Pair Carbs with Protein: Eating dal with rice or paneer with roti slows down glucose absorption.
Policy and the Future: Where Do We Stand?
The government has recognised the threat. The Economic Survey 2025-26 suggested exploring fiscal measures to curb the consumption of unhealthy, ultra-processed foods (UPFs) by proposing the highest GST slab on such items.
However, a gap exists between intent and action. While Budget 2026 focused on big-ticket scientific initiatives, public health experts note a "disconnect" with the Economic Survey's aggressive recommendations. The increase in health allocations has been modest, and schemes like Jan Aushadhi (which provides affordable medicines) have seen funding fluctuations.
For the average Indian, this means that while the future of drug manufacturing appears bright (thanks to Biopharma Shakti), the immediate need for preventive services and primary healthcare strengthening remains urgent.
Hope on the Horizon
Despite the grim statistics, immense hope exists. We stand at a point in history where technology, policy, and awareness are converging.
Technology: From Continuous Glucose Monitors (CGMs) that display real-time sugar levels to AI-driven diagnostics, technology is empowering patients. The 2026 Budget's push for AI integration in healthcare aims to provide structural reforms that will shape India's future health landscape.
Telemedicine: Platforms are making expert consultations accessible in small towns, helping bridge the urban-rural divide.
Traditional Knowledge: There is renewed interest in millets and traditional grains. The government's push for Ayurveda and the integration of traditional medicine with modern research could unlock new, sustainable ways to manage metabolic health.
Conclusion: The Fight Begins at Home
Diabetes is indeed the biggest threat to mankind, and for India, it represents a clear and present danger. It threatens to consume our healthcare budget, drain our economy, and orphan our children. But it is not an invincible foe.
The weapons to defeat it are simple: awareness, diet, exercise, and community support. We must create a movement where checking blood sugar becomes as normal as checking blood pressure. We must demand healthier food environments from our policymakers. We must revive our traditional dietary wisdom that kept our ancestors healthy.
If you are reading this and you have a family history of diabetes, or if you are overweight, or if you lead a sedentary life, consider this your wake-up call. Get tested. If you have prediabetes, know that it is reversible. If you have diabetes, know that with disciplined management, you can live a long, healthy, and productive life.
The biggest threat to mankind is not the disease itself, but our inaction in the face of it.
Let us act now.

